


Fact Sheet
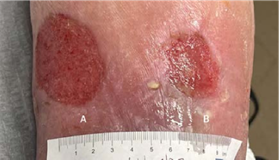
(A) Wound resolved
(B) 1.5 x 1 x 0.1 cm
Volume reduced: 70%
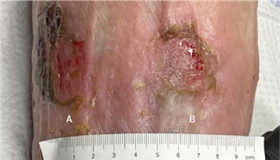
WEEK 3 Patient is improving; a third 4 x 4 cm Impax is applied, after which wounds are completely healed at fourth week follow-up
(A) 3 x 1.8 x 0.1 cm
Volume reduced: 80%
(B) 2.5 x 2 x 0.1 cm
Volume reduced: 33.3%
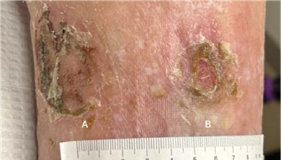
WEEK 2 Patient tolerating Impax well; a second 4 x 8 cm Impax is applied
(A) 6 x 4.5 x 0.1 cm
(B) 2.5 x 3 x 0.1 cm
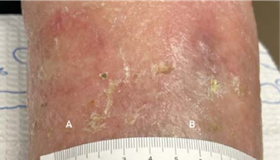
WEEK 1 After sharp excisional debridement, application of4 x 8 cm Impax.
(A) 6 x 4.5 x 0.1 cm,
(B) 2.5 x 3 x 0.1 cm
INITIAL VISIT Incision, draining, and debridement, with Impax to be applied at next follow-up

(A) 0.9 x 0.8 x 0.3 cm
(B) 4.6 x 3.3 x 0.2 cm
(C) 2 x 1.2 x 0.3 cm
INITIAL VISIT Post-debridement applied 2 x 2 cm Impax to all wounds

(A) 0.2 x 0.3 x 0.2 cm
Volume reduced: 94%
(B) 1.1 x 0.5 x 0.2 cm
Volume reduced: 96%
(C) 0.6 x 0.8 x 0.3 cm
Volume reduced: 80%
2-WEEK VISIT Post-debridement applied 2 x 2 cm Impax to all wounds

(A) Wound resolved
(B) 1.8 x 0.4 x 0.1 cm
Volume reduced: 35%
(C) 0.3 x 0.6 x 0.3 cm
Volume reduced: 63%
6-WEEK VISIT After surgery to remove infected bone and resolution of infection; post-debridement applied 2 x 2 cm Impax to all wounds

(B) 1.1 x 0.4 x 0.1 cm
Volume reduced: 39%
(C) 0.3 x 0.4 x 0.2 cm
Volume reduced: 56%
8-WEEK VISIT Post-debridement applied 2 x 2 cm Impax to all wounds

(B) 0.5 x 0.1 x 0.1 cm
Volume reduced: 89%
(C) 0.6 x 1 x 0.2 cm
Volume increased: 400%
10-WEEK VISIT Post-debridement applied 2 x 2 cm Impax to all wounds
(B) Wound resolved
(C) 0.4 x 0.6 x 0.3 cm
Volume reduced: 40%
12-WEEK VISIT Post-debridement applied 2 x 2 cm Impax to wound; all wounds resolved at week 13